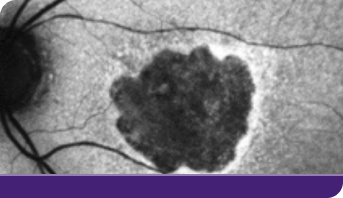
Geographic atrophy, or GA, can progress quickly and unpredictably, and your patients are at risk of losing vision each day.1 Taking action to potentially buy more time with their remaining vision matters to your patients.
In a survey of people with self-reported GA, 84% said they would try a treatment to slow GA and preserve their vision for longer, but only 14% receive treatment.2,3 Preserving your patients' vision is more than just their sight, it's about potentially protecting how your patients' may visually experience life for longer.
Hi, I’m Arshad Khanani, Director of Clinical Research and Director of Fellowship at Sierra Eye Associates, and Clinical Professor at the University of Nevada, Reno School of Medicine. Today I want to talk to you about IZERVAY™ (avacincaptad pegol intravitreal solution): a tool that we can use to protect patients’ healthy retinal cells for longer by slowing down the progression of GA.
IZERVAY is indicated for the treatment of geographic atrophy secondary to age-related macular degeneration, or AMD.4 IZERVAY is contraindicated in patients with ocular or periocular infections and in patients with active intraocular inflammation.4 Please see additional safety information at the end of the video.
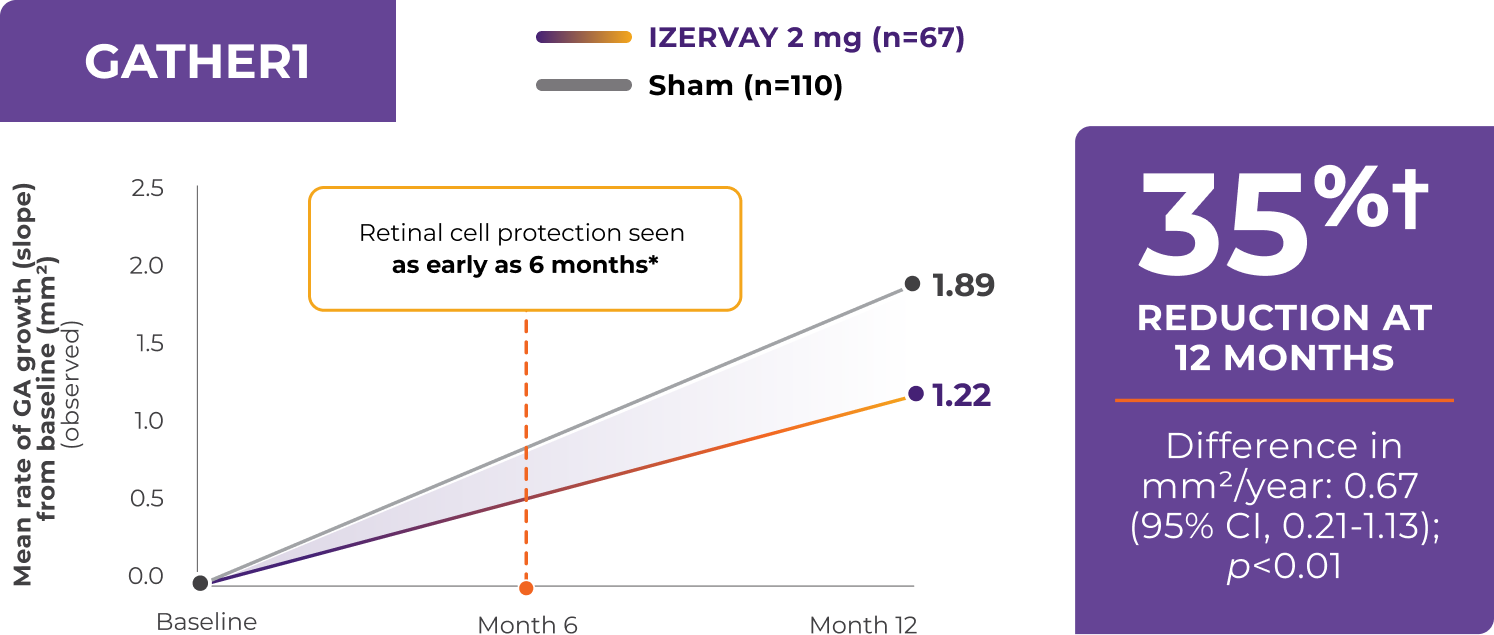
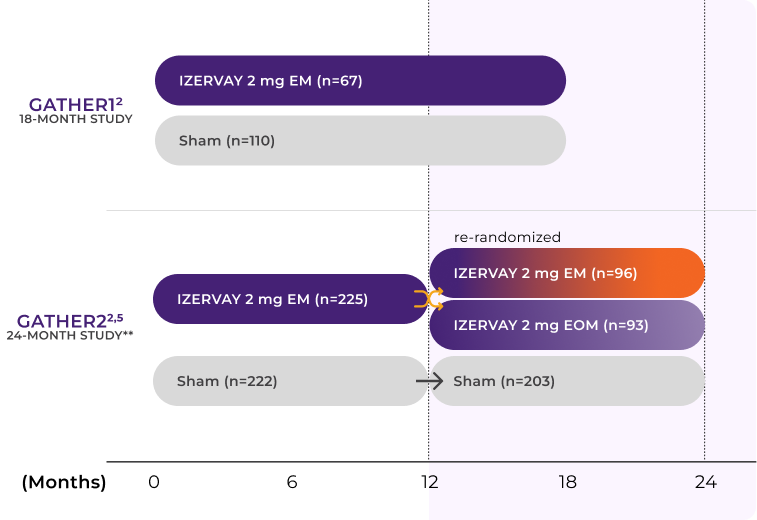
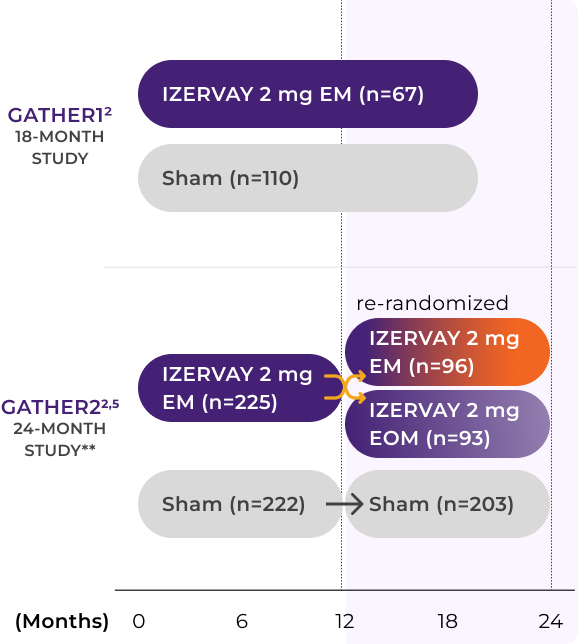
IZERVAY was studied in patients with GA due to AMD in two randomized, multicenter Phase 3 trials: GATHER1, over 18 months, and GATHER2, over 24 months, with 624 patients across both trials.4-7 Both GATHER1 and GATHER2 were designed to evaluate the efficacy and safety of IZERVAY compared to sham with a primary endpoint at 12 months and additional long-term analyses conducted at 18 and 24 months.4
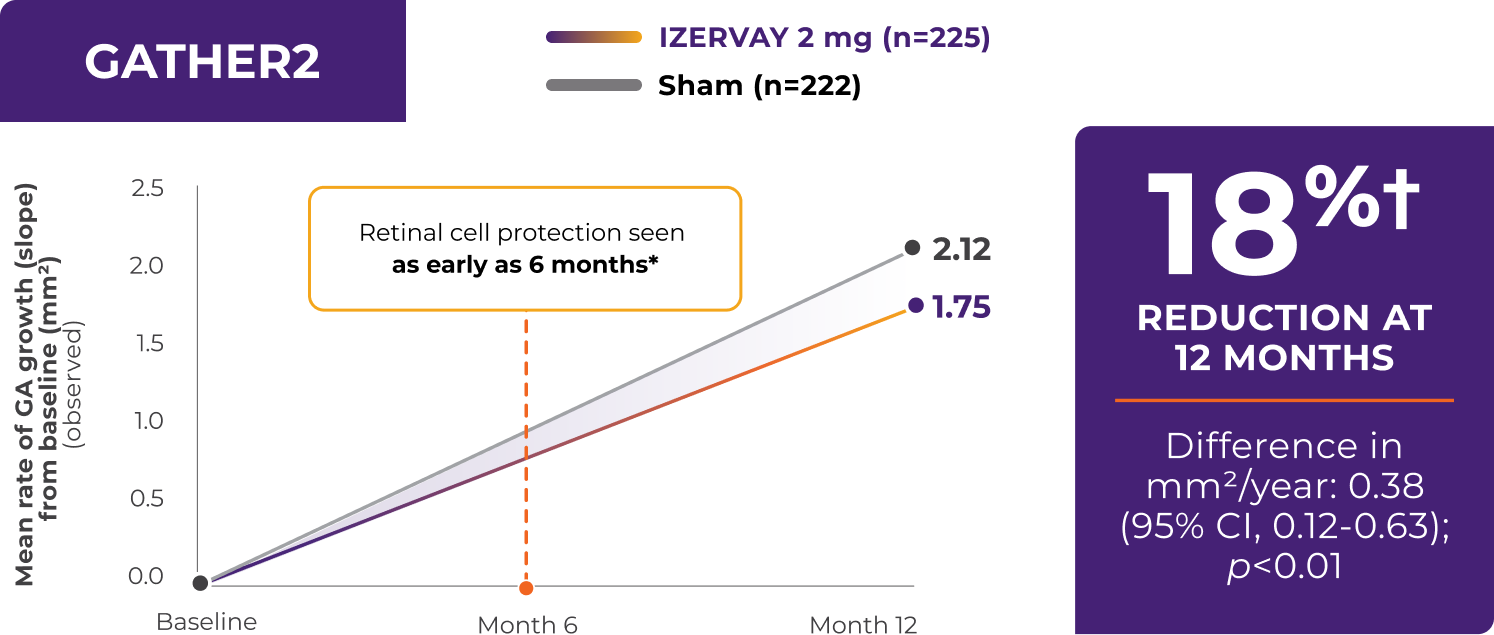
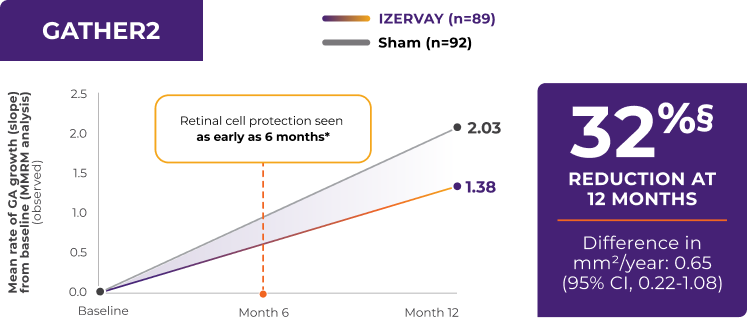
At the 12-month time point, IZERVAY achieved its primary clinical endpoints in both the GATHER1 and GATHER2 trials, demonstrating stat significant protection of healthy retinal cells within the first year of treatment with a 35% and 18% reduction in the annualized rate of GA growth in the GATHER trials.4 It is important to note that IZERVAY is the only GA treatment to demonstrate stat significant efficacy at one year in two Phase 3 trials.8 In addition to this early efficacy within the first year, IZERVAY started protecting healthy retinal cells as soon as 6 months. As you see through this 12-month timeframe, IZERVAY’s effect continued to grow in its separation from sham. This trend continued through 24 months.4 Let’s go there next.
When we look at the 24-month clinical data from GATHER2, IZERVAY demonstrated a 14% reduction in the annualized rate of GA growth with an increasing and doubling effect from baseline to 24 months compared to baseline to 12 months. At first glance, you may ask yourself how there could be a doubling effect when the results from GATHER2 year 1 showed an 18% annualized reduction in growth rate and GATHER2 across 24 months showed a 14% annualized reduction.4,9 Let’s take a closer look.
In GATHER2, patients receiving monthly IZERVAY were re-randomized at Month 12 to either continue monthly dosing or transition to every-other-month dosing.4 This re-randomization created two distinct treatment subgroups within the active arm for the second year of the study. As a result, new slopes for each subgroup needed to be recalculated from baseline to 24 months. Because this calculation separates the data into two distinct dosing regimens, monthly or every-other-month, we need to look at each treatment group in comparison to itself. In conclusion, the addition of different subgroups make it difficult to compare Year 1 and Year 2 data, which is why an annualized rate was calculated.4
Additionally, when we look at the piecewise analysis, which helps us understand how the treatment effect varies across 6-month time periods, we observe that the treatment effect more than doubled over the full 24 months as compared to the first 12 months.9 What makes the 24-month data meaningful is that it demonstrated a cumulative and increasing treatment effect over time. We see in the data that the separation between IZERVAY treatment groups versus sham continued to widen beyond Month 12, indicating that the treatment effect not only persisted, it increased over time.5
Now let's take a look at IZERVAY’s safety profile as demonstrated in the GATHER trials. IZERVAY is the only FDA-approved GA treatment with no warning or precaution for intraocular inflammation or retinal vasculitis.4,10 In the GATHER1 and GATHER2 trials, at 12 months, we saw a slight increase in neovascular wet AMD or choroidal neovascularization in patients treated with IZERVAY compared to the sham group. The rate was 7% in the IZERVAY treated group versus 4% in the sham group. In GATHER2, over 24 months, the rate of neovascular wet AMD or choroidal neovascularization was 12% with IZERVAY and 9% with sham.4,9 Safety findings through 24 months in patients with GA secondary to AMD were consistent with those observed at 12 months.5,6,9
We know that patients with GA will progress over time, but with IZERVAY, we have the potential to help our patients preserve their vision for longer.1 IZERVAY is the only GA treatment to demonstrate stat significant efficacy at one year in two Phase 3 trials.4,8 It also starts working early with efficacy demonstrated within the first year, and has continued to show an increasing treatment effect over time.4,9
As a physician, I’m looking at the totality of the data, and that’s why IZERVAY is my choice for my patients with GA. It’s time to close that gap between the 84% of patients with GA who desire treatment and the 14% who actually receive it.
INDICATION
IZERVAY™ (avacincaptad pegol intravitreal solution) is indicated for the treatment of geographic atrophy (GA) secondary to age-related macular degeneration (AMD)
IMPORTANT SAFETY INFORMATION
CONTRAINDICATIONS
IZERVAY is contraindicated in patients with ocular or periocular infections and in patients with active intraocular inflammation.
WARNINGS AND PRECAUTIONS
Endophthalmitis and Retinal Detachments
- Intravitreal injections, including those with IZERVAY, may be associated with endophthalmitis and retinal detachments. Proper aseptic injection technique must always be used when administering IZERVAY in order to minimize the risk of endophthalmitis. Patients should be instructed to report any symptoms suggestive of endophthalmitis or retinal detachment without delay and should be managed appropriately.
Neovascular AMD
- In clinical trials, use of IZERVAY was associated with increased rates of neovascular (wet) AMD or choroidal neovascularization (7% when administered monthly and 4% in the sham group) by Month 12. Over 24 months, the rate of neovascular (wet) AMD or choroidal neovascularization in the GATHER2 trial was 12% in the IZERVAY group and 9% in the sham group. Patients receiving IZERVAY should be monitored for signs of neovascular AMD.
Increase in Intraocular Pressure
- Transient increases in intraocular pressure (IOP) may occur after any intravitreal injection, including with IZERVAY. Perfusion of the optic nerve head should be monitored following the injection and managed appropriately.
ADVERSE REACTIONS
Most common adverse reactions (incidence ≥5%) reported in patients receiving IZERVAY were conjunctival hemorrhage, increased IOP, blurred vision, and neovascular age-related macular degeneration.
Please see full Prescribing Information on IZERVAYecp.com.
References
1. Fleckenstein M, Mitchell P, Freund KB, et al. The progression of geographic atrophy secondary to age-related macular degeneration. Ophthalmology. 2018;125(3):369-390. 2. Bakri SJ, Brinkmann CK, Mulvey A, et al. Characterizing patient perceptions of living with geographic atrophy: the global Geographic Atrophy Insights Survey. Clin Ophthalmol. 2024;18:3725-3737. 3. Astellas Pharma US, Inc. Izervay. Data on File. 4. Izervay. Package insert. Northbrook, IL: Astellas Pharma US, Inc.; 2025. 5. Patel SS, Lally DR, Hsu J, et al. Avacincaptad pegol for geographic atrophy secondary to age-related macular degeneration: 18-month findings from the GATHER1 trial. Eye (Lond). 2023;37(17):3551-3557. 6. Khanani AM, Patel SS, Staurenghi G, et al. Efficacy and safety of avacincaptad pegol in patients with geographic atrophy (GATHER2): 12-month results from a randomised, double-masked, phase 3 trial. Lancet. 2023;402(10411):1449-1458. 7. Clinical Trials.gov. Zimura in Participants With Geographic Atrophy Secondary to Age-Related Macular Degeneration. Accessed August 14, 2025. https://clinicaltrials.gov/study/NCT02686658 8. Heier JS, Lad EM, Holz FG, et al. Pegcetacoplan for the treatment of geographic atrophy secondary to age-related macular degeneration (OAKS and DERBY): two multicentre, randomized, double-masked, sham-controlled, phase 3 trials. Lancet. 2023;402(10411):1434-1448. 9. Astellas Pharma US, Inc. Izervay. Data on File. 10. Syfovre. Package Insert. Waltham, MA: Apellis Pharmaceuticals. 2025.